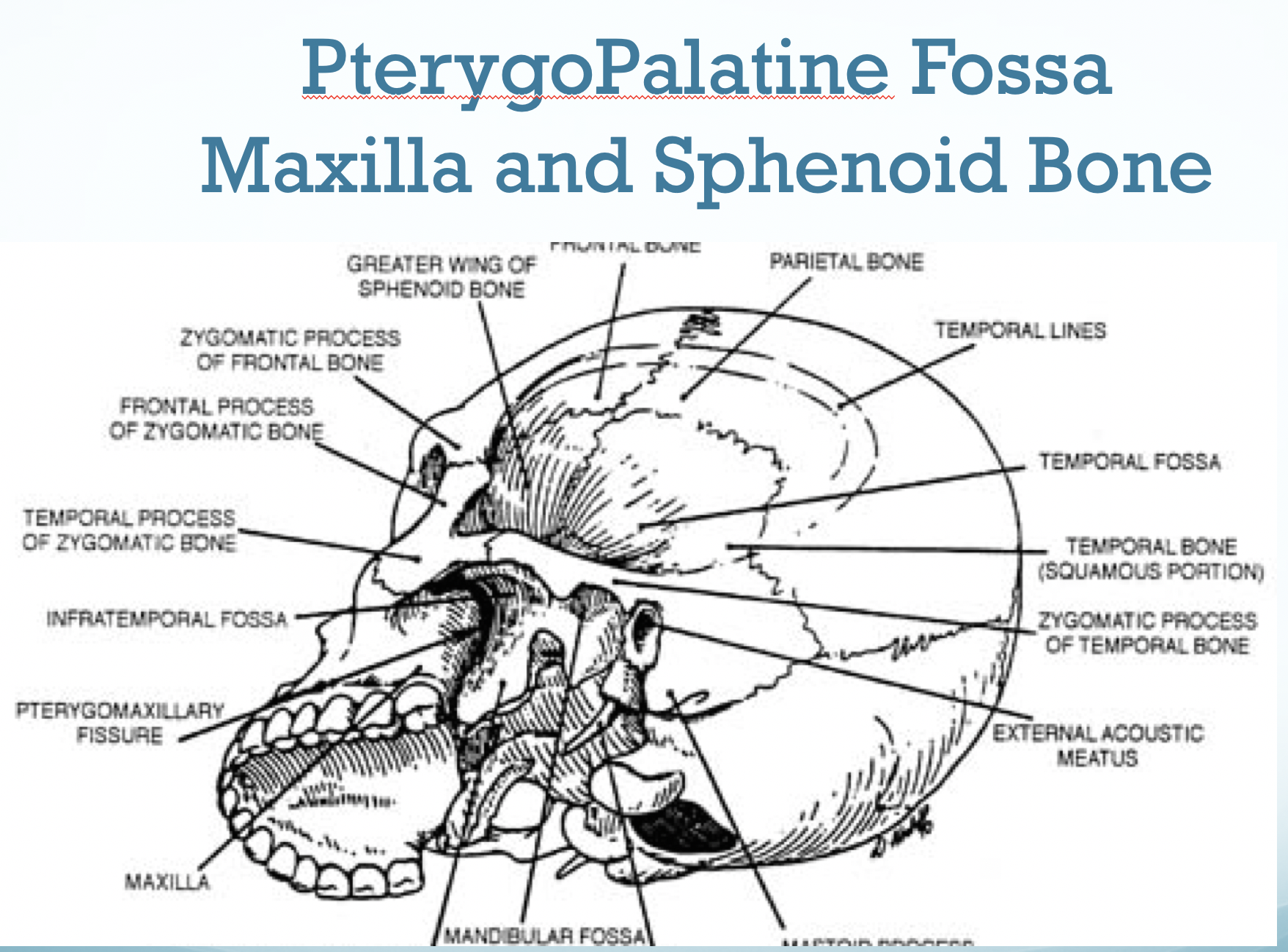
The PterygoPalatine Ganglion is found in the Pterygoid Fossa. The Pterygopalatine Ganglion is Commonly called the Sphenopalatine Ganglion or SPG.
Sphenopalatine Ganglion Blocks: A Game Changer in the treatment, management and elimination of chronic headaches and migraines.
Chronic migraine and severe headaches are common conditions that adversely affect all aspects of Quality of Life (QOL). No available treatments are universally effective and many carry risks of side effects. Sphenopalatine Ganglion Blocks when effective take effect within inutes and negative side effects are virtually nonexistent.
Blockade of the sphenopalatine ganglion (SPG) nerve has over a 100 year amazing safety record. There are multiple approaches to Sphenopalatine Ganglion Blocks but the first one described in 1908 by Dr Greenfield Sluder was application of an intranasal topical anesthetic. In 1930 an article in Annals of Internal Medicine (JAMA) by Dr Hiram Byrd documented 10,000 blocks in 2000 patients without significant side effects.
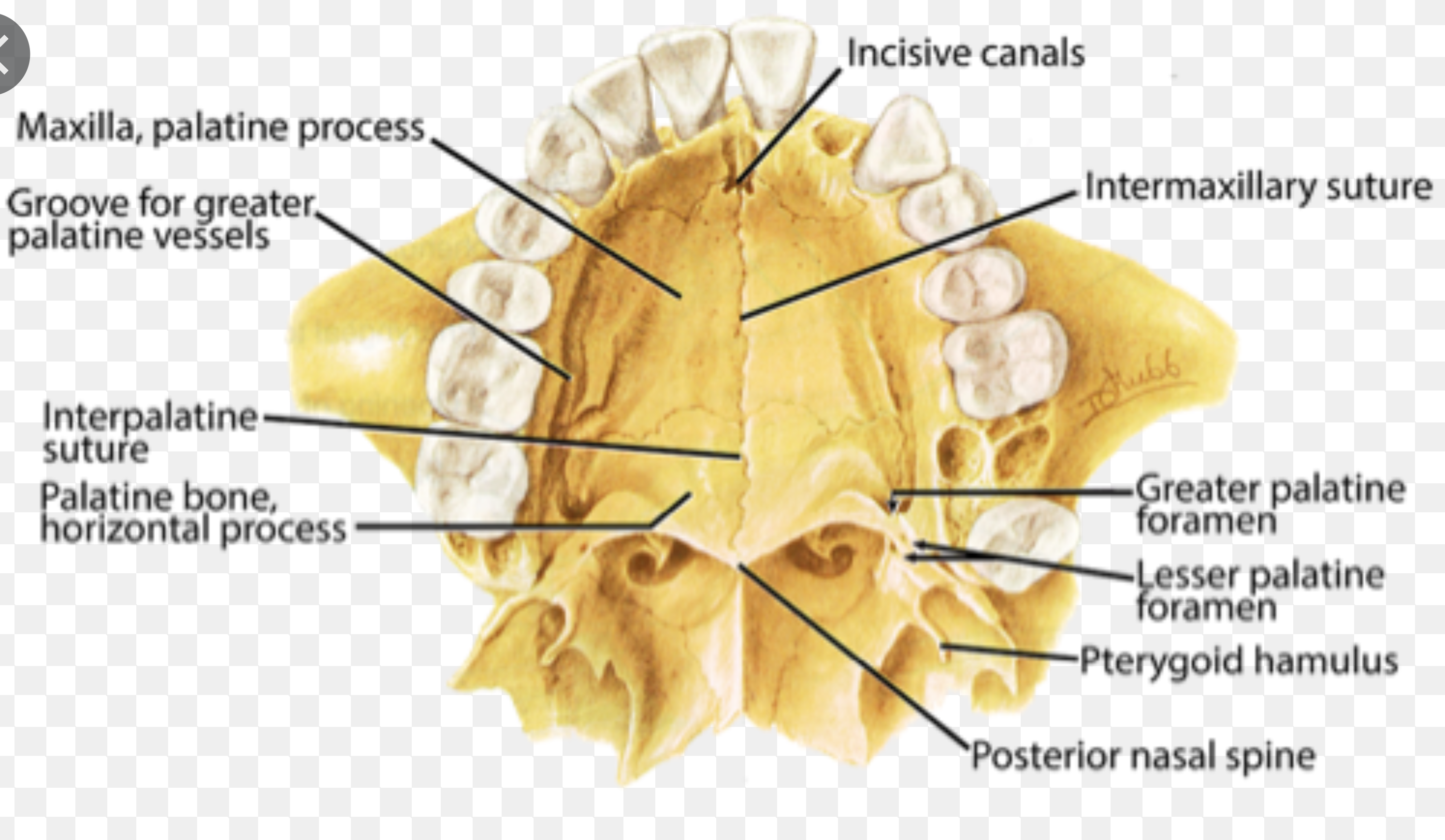
There are multiple injection approaches to blockage of the Sphenopalatine Ganglion including both intra-oral and extra-oral approaches. The Greater Palatine Foramen is an intra-oral blockand is often used in dentistry especially for upper molar root canals and extractions. Dentists are the experts on this block. Extraoral injections of the SPG can be done with a lateral approach thru the masseter muscle or via a Suprazygomatic Approach.
THE GREATER PALATINE FORAMEN IS UTILIZED FOR INTRAORAL SPHENOPALATINE GANGLION BLOCK
The U.S. Food and Drug Administration (FDA) has approved multiple Nasal Catheter devices for delivering Sphenopalatine Ganglion Blocks trans-nasally or through the nares..
The Sphenopalatine Ganglion (SPG) is also called by multiple other names including the Pterygopalatine Ganglion named for its position in the Pterygopalatine Fossa and the Nasal Ganglion named for position and access thru the nose. It was originally called Sluder’s Ganglion after Dr Greenfield Sluder who first described the use of Nasal Blocks. It is als known as Meckel’s Ganglion and Maxillary Ganglion.
THE PTERYGOPALATINE FISSURE IS WHERE EXTRAORAL SPHENOPALATINE GANGLION BLOCK IS DIRECTED.
THIS CAN BE A LATERAL APPROACH OR PREFERRED SUPRAZYGOMATIC APPROACH UTILIZING 50 MM NEEDLE.
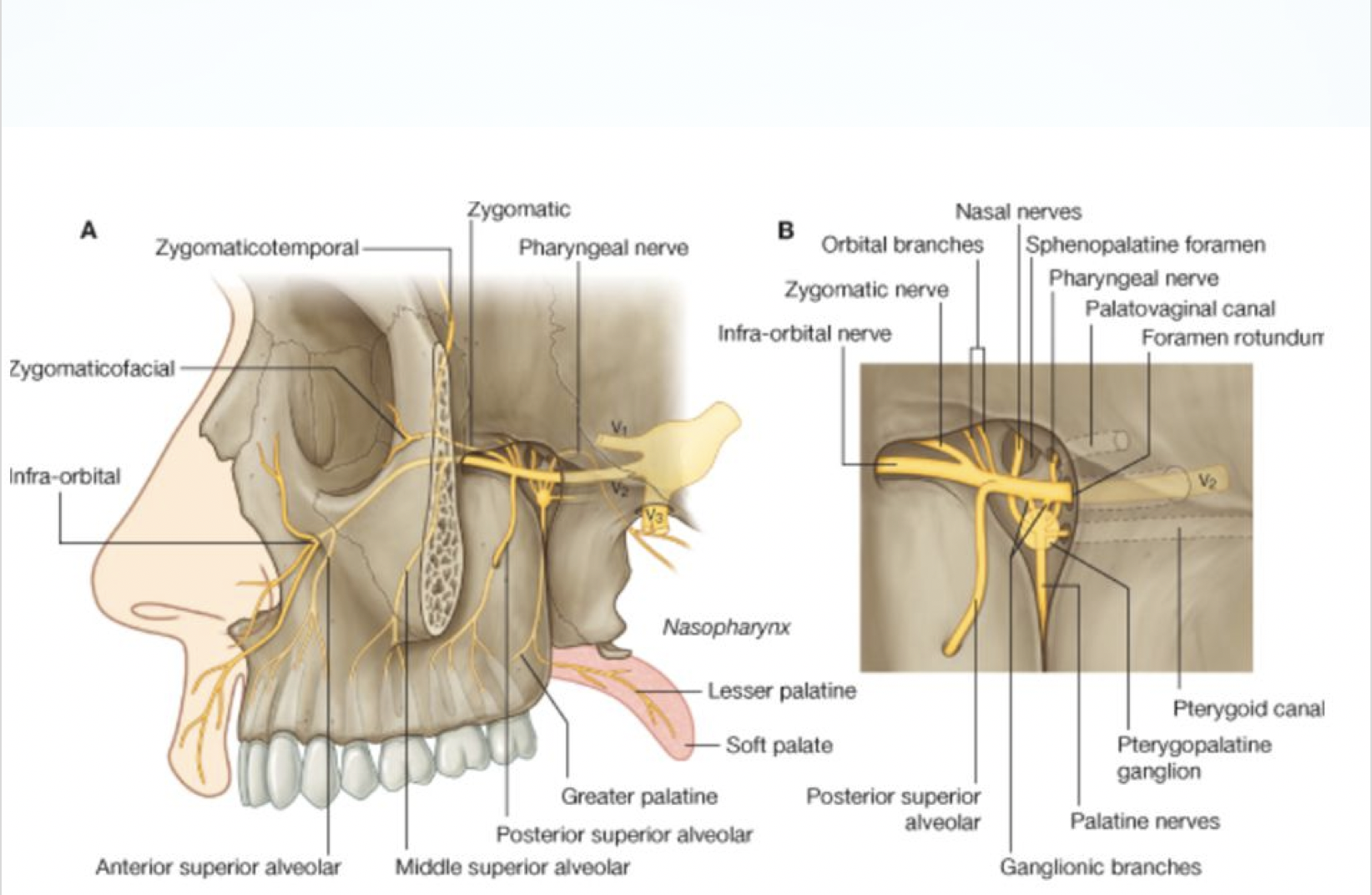
The Sphenopalatine Ganglion is the Largest Parasympathetic Ganglion of the Cranium and it also carries Post Ganglionic Sympathetic Fibers from the Superior Sympathetic Chain. It is directly connected to the Maxillary Division of the Trigeminal Nerve and supplies Sympathetic and Parasympathetic fibers to all Trigeminal Nerve branches.
The Sphenopalatine Ganglion Block has been called “The Miracle Block” after the publication of “Miracles on Park Avenue” about the work of Milton Reder and seemingly “Miracle Cures” utilizing only Sphenopalatine Ganglion Blocks. The Pterygopalatine Ganglion has been called “The Piccadilly Circus of the Face”. Drs Benzaart, Smith and Reyneke utilized this term in their book Pterygopalatine Ganglion Blocks for Effective Treatment of Migraine, Cluster and Postdural Puncture Headache and Post Operative Pain. Shenopalatine Ganglion (SPG) Blocks and Pterygopalatine Ganglion blocks are identical.
When Sphenopalatine Ganglion Blockage relieves or prevents headaches or migraines it is diagnostic of an autonomic component to these headaches. Due to the safety and effectiveness in prophylactic prevention and treatment it should be considered an important part of the diagnostic work-up in all headache patients. Response to the block is indicative of the autonomic contribution to the headache or migraine.
HEADACHES AND HEADACHE TREATMENTS
Headaches are commonly thought of as neurologic /vascular disorders though they are often referred from Myofascial Trigger Points and other tissues. Headaches are one of the top reasons why patients seek medical care.
Headaches are so common that they affect at least 50% of the general population in any given year. More than 90% of the population have a lifetime history of headache.
Tension-type headaches and migraines are the two most common types of headaches but differential diagnosis and testing of actual headache causes are often lacking.
Diagnostic criteria for tension headaches include the presence of at least two of the following characteristics: bilateral (typical but not universal) headache location, non-pulsating pain, mild to moderate (can be severe in some patients) intensity. Tension type headaches are frequently referred myofascial headaches. The use of Travell Spray and Stretch with Vapocoolant spray to deactivate trigger points is often used to treat these headaches and as part of a diagnostic protocol. Relief of headaches with Travell Spray and Stretch is diagnostic of Myofascial referred headaches, the most common type of tension headaches. Myofascial pain often serves as a trigger for other types of headaches including migraine. Elimination of myofascial trigger points can lead to decrease or elimination of secondary migraines. Unfortunately most headaches are treated by neurologists who often have minimal understanding of this critical information. Physiatrists, Physical Therapists and Dentists who treat Temporomandibular Dysfunction typically have the best understanding of myofascial causes of pain.
Migraines are the second-most common headache disorder. Severe headaches are often routinely diagnosed as migraines incorrectly. Frequently the diagnosis of “Migraine” can actually become an obstacle to finding the best treatments. Migraines are characterized by severe pain on one or both sides of the head, possible nausea, and/ or disturbed vision. Migraines can be categorized by headache frequency, and by the presence or absence of aura. Chronic migraines are defined as attacks at least 15 days per month for more than 3 months, with features of migraine at least 8 days per month.
Cluster headaches (a Trigeminal Autonomic Cephalgia) are less common than tension or migraine headaches. They are characterized by severe unilateral orbital, supraorbital, and/or temporal pain that also includes other symptoms in the eye and/or nose on the same side (e.g., rhinorrhea, eyelid edema or drooping). Elimination of pain with administration of 100% oxygen is considered diagnostic for a cluster headache though that treatment is not universally successful.
A wide variety of medications are used to treat acute migraine episodes or prophylactically stop migraines at their onset including triptans and ergotamines and other medications that treat the pain and other symptoms of migraines once they are established (nonsteroidal anti-inflammatory drugs, antiemetics.
Prophylactic medication therapy is often utilized for people with migraines that occur more than 2 days per week. The use of 2% Lidocaine delivered to the Sphenopalatine Ganglion by Self-Administration with Cotton-Tipped Catheters can not only prevent attacks but can also be utilized to decrease pain or eliminate the pain of an acute attack. Frequency of administration of Self-Administered SPG Blocks(SASPGB) my vary by patients and there is evidence that efficiency in increased by increased frequency of administrationdition to medication, behavioral treatments (eg, relaxation, cognitive therapy) are used to manage migraine headache. Botulinum toxin type A injections are an FDA‒approved treatment for chronic migraine though there is evidence that it spreads to the brain over time. Severe acute cluster headaches may be treated with abortive therapy including breathing 100% oxygen, and triptan medications. Other medications used to treat cluster headaches include steroids, calcium channel blockers, and nerve pain medications. Due to the severity of pain associated with cluster headaches, patients may seek emergency treatment. Cluster Headaches frequently send patients to the Emergency Department where medical costs spiral. Patients who benefit from Self-Administered SPG Blocks (SASPGB) can vastly improve quality of life by avoiding costly medical visits and more importantly receiving faster pain relief with less negative side effects.
THE COTTON-TIPPED CATHETER DELIVERS CONTINUAL CAPILLARY FLOW TO MUCOSA OVER PTERYGOPALATINE FOSSA & SPG
Tension-type headaches are generally treated with over the counter pain medication. This is often problematic due to GI issues associated with NSAIDS. The use of Travell Spray and Stretch that is used to diagnose the myofascial orgin of headache pain can often be taught to patients who can utilize it to eliminate/decrease headache pain almost instantly. Myofascial Pain is often secondary to repetitive strain injury of the jaw, head and neck musculature and elimination of underlying causes can effectively eliminate much of this pain. Neuromuscular Dentistry is extremely effective an idealizing muscle function related to jaw function.
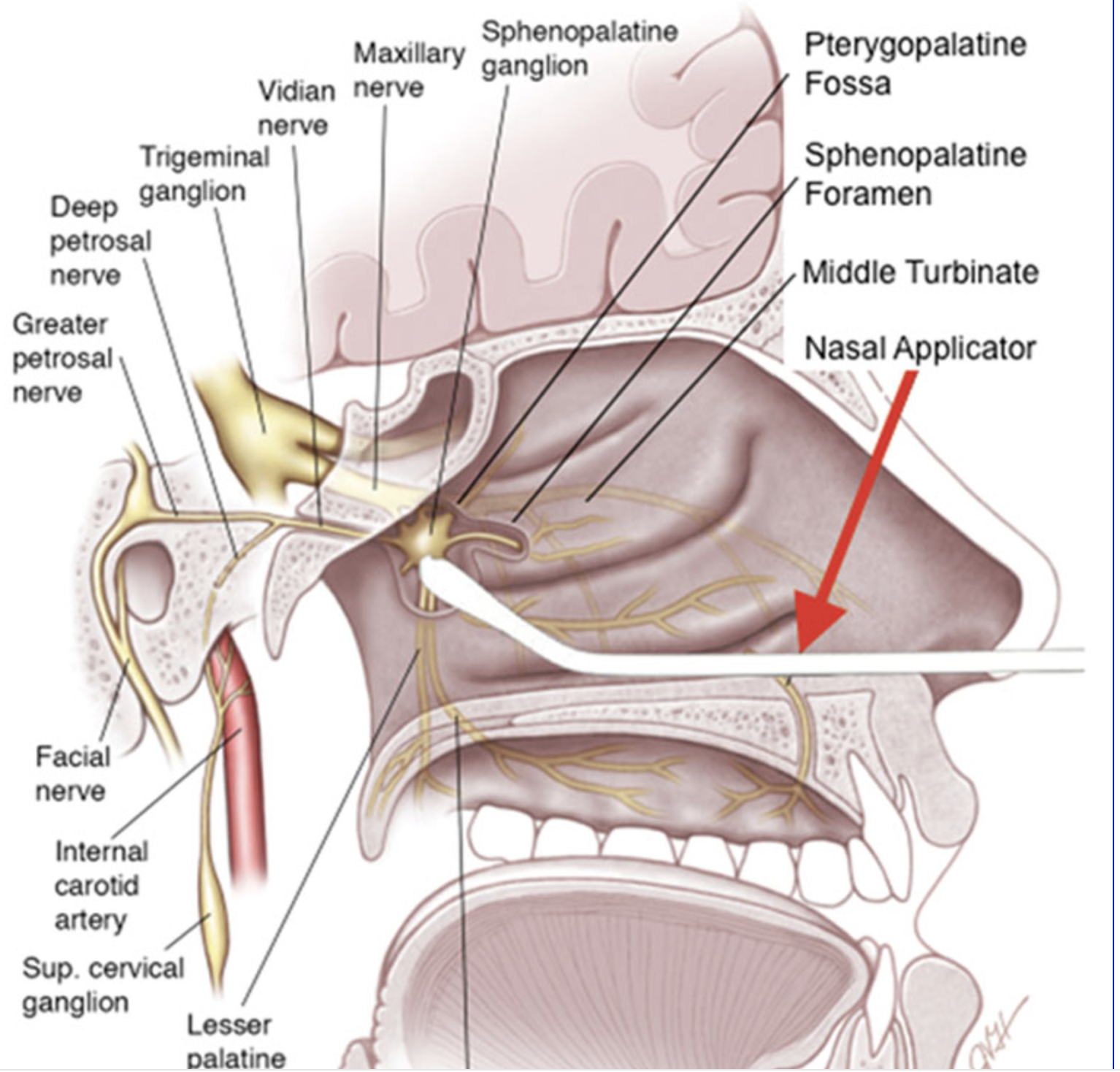
The Sphenopalatine Ganglios has both autonomic nerves and somatosensory nerves, which are associated with functions such as tearing and nasal congestion, and sensory nerves, associated with pain perception. Trans-nasal SPG blocks involve topical application of local anesthetic to mucosa overlying the SPG. One rationale for using SPG blocks to treat headaches is that local anesthetics in low concentrations could block the sensory fibers and thereby reduce pain while maintaining autonomic function a second rationale is that the headaches and migraines are autonomically maintained via General Autonomic Visceral afferents. The SPG Block may actually act as a reset mechanism similar to hitting Control/Alt/ Delete to reset a computer issue.
One procedure for SPG blockade is to insert an intranasal catheter that is attached to a syringe carrying local anesthetic (e.g., lidocaine, bupivacaine). Once the catheter is in place, the local anesthetic is applied to the posterior/lateral wall of the nasal cavity, reaching the mucosa overlying the pterygopalatine fossa where the Pterygopalatine (SPG) Ganglion is located. These devices are essentially “Squirt Guns” and only offer a short exposure of the anesthetic to the mucosa. The use of Cotton-tipped catheters for Self-Administration is a far more effective approach as there is a continual capillary feed of anesthetic to the mucosa overlying the pterygopalatine Fossa and the Sphenopalatine Ganglion. Because of the continual capillary action release the area is bathed in 2% lidocaine over an extended period of time. There is less anesthetic in the throat and the lidocaine is a natural anti-inflammatory agent.
Most important is the convenience and extremely low cost of Self-administration. The ease of the blocks mean that patients can avoid expensive ER visits and unnecessary physician visits. This is especially important during the Covid 19 pandemic where social distancing is paramont. The Self-Administered SPG Blocks are also effective for treating anxiety and stress a common symptom in all headache patients as well as during this pandemic.
Originally, SPG blocks were done by inserting a cotton-tipped applicator dabbed with local anesthetic into the nose as described by Sluder in 1908. The original anesthetic agent used was cocaine but 2% lidocaine is very effective. The use of cotton-tipped catheters is a major improvement over the solid cotton tipped applicator that did not give continual capillary feed. The continual feed allows a wide spread of the lidocaine thru the tissue so it is more forgiving in placement. Patients do need to be taught proper placement and tricks to make the process easier and more comfortable. Laying supine with the cotton-tipped catheter will increase the rate of dispersion due to the pull of gravity. The ability to go thru all activities of daily living while Self-administering SPG Blocks is a key to patient comfort and usage. Patients can eat, drink, cook, work on computers or watch TV. They are almost unlimited in daily functions.
LEARN TO SELF-ADMINISTER SPG BLOCKS WITH DR SHAPIRA
Chicago: Learn How to Self-Administer Sphenopalatine Ganglion Blocks
There are three FDA approved catheter devices are commercially available in the United States for physicians performing SPG blocks. The catheters have somewhat different design but all are attached to syringes that contain local anesthetic. The catheters are inserted intranasally and, once in place, the local anesthetic is applied through the catheter. With 2 of the 3 commercially available catheters (the SpenoCath®, Allevio™), patients are Typically positioned on their back with their nose pointed vertically and their head turned to the side. They stay in that position for 20 minutes and if bilateral blocks are performed ideally 20 minutes on each side. Wihen using the Tx360® device, patients remain seated but ideally they would likely improve outcomes by following the same protocol as the other devices..
The MiRX™ protocol combines SPG Blocks with the Tx360® device wirh a medical component for immediate pain relief and a physical component to reduce headache recurrences. This is exactly the type of protocol used with the Self-Administration protocol combining physical activity and myofascial treatment with SPG Blocks in a more convenient method that is life style friendly for patients.
Patients undergoing Neuromuscular approach to dealing with the repetitive strain injuries will related to TMJ disorders (TMD) often utilize SPG Blocks with neuromodulation of the Sphenopalatine Ganglion. These doctors utilize an ULF-
TENS that also acts as a muscle stimulation and neuromodulation of the Sphenopalatine Ganglion and the trigeminal nerve, both sensory
Division V(afferent) and motor division (efferent) and effectively correct many myofascial issues of masticatory and cervical muscles.
https://www.sphenopalatineganglionblocks.com/tag/spg-blocks-cost/